คนไข้ปฏิเสธการผ่าตัดขากรรไกร เราจึงต้องบูรณาการความรู้ที่มี ช่วยน้องคนไข้
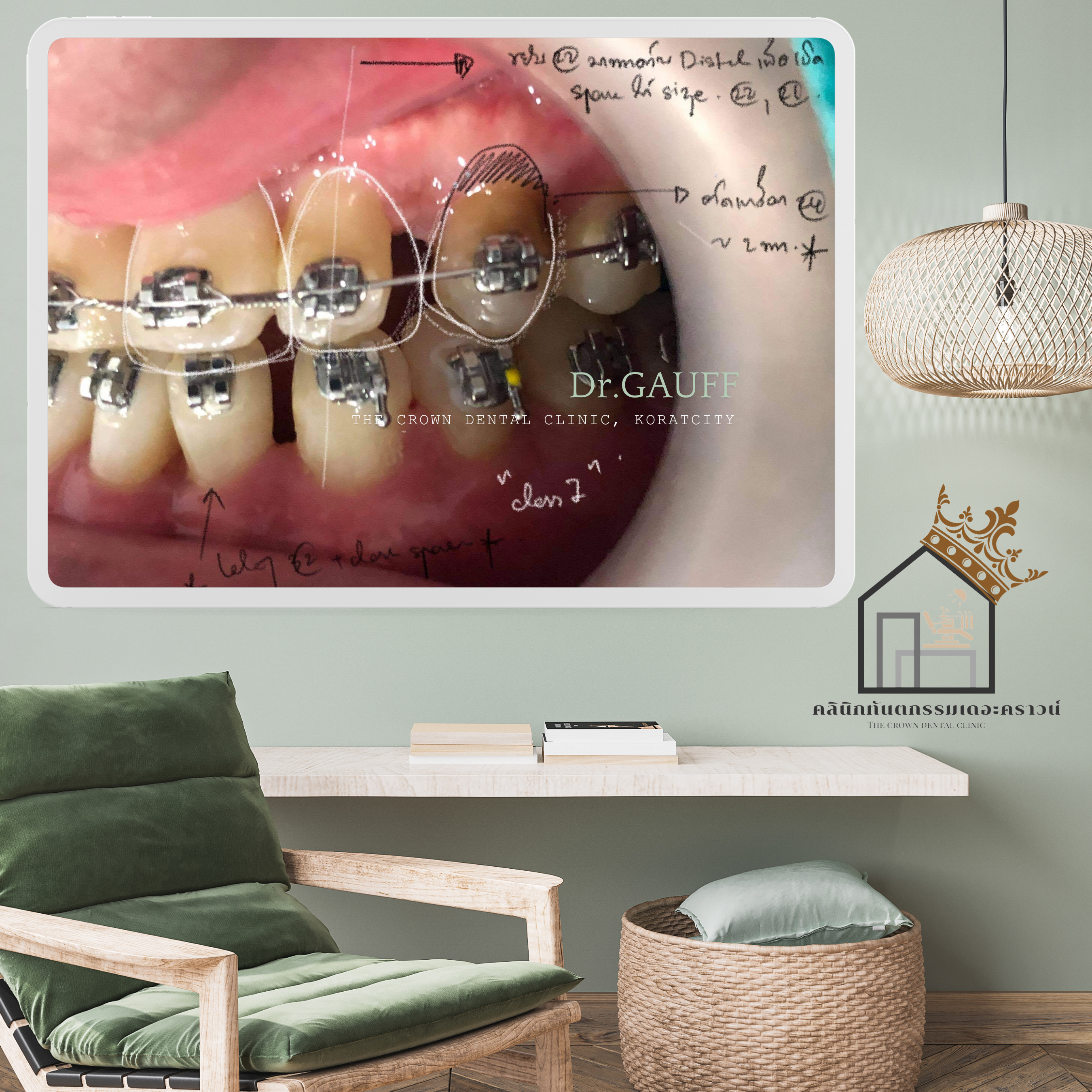
รีวิวเคสจัดฟันของคลินิกทันตกรรมเดอะคราวน์ โคราช เป็นเคสที่คนไข้มีความผิดปกติของขากรรไกรบนที่เล็กกว่าปกติ และเป็น V-Shape ร่วมกับฟันหน้าล่าคร่อมฟันหน้าบน (สบฟันหน้าไขว้ หรือ Anterior Cross Bite) มีฟันหน้าซ้อนทั้งบนและล่าง แนวฟันหน้าล่างล้มเข้าด้านลิ้นตั้งแต่ก่อนเริ่มรักษา และยังตรวจพบฟันซี่เขี้ยวด้านซ้ายบนฝัง
อธิบายทุกความเสี่ยงที่อาจจะต้องเจอทั้งระหว่างการจัดฟัน และหลังการจัดฟัน จริงๆความผิดปกติมาจากกระดูก การแก้ไขด้วยการศัลยกรรมกระดูกขากรรไกร ร่วมกับการจัดฟัน น่าจะเป็นทางแก้ไข เพื่อสร้างการสบฟันในตำแหน่งที่ดีกว่าการเลือกรักษาเพียงแค่การจัดฟัน แต่หากคนไข้ปฏิเสธการผ่าตัด การจัดฟันเพียงอย่างเดียวย่อมมีความเสี่ยง เช่นฟันหน้าล่างงุ้มมากกว่าปกติ หรือการเหลือช่องว่าง ต้องได้รับการแก้ไขด้วยการอุดแต่ง หรือการทำวีเนียร์ต่อหลังการจัดฟันเสร็จ



เมื่อเรียงฟัน และแก้ระนาบการสบฟันให้มีการสบที่มีเสถียรภาพแล้ว ก็มาวางแผนการจัดการช่องว่างที่เหลือ จากการถอนฟันที่ซ้อนเกมากๆออก โดยแก้ไขช่องที่เกิดขึ้นด้วยการอุดแต่งในระหว่างการจัดฟัน และเมื่อการจัดฟันเสร็จสิ้น แนะนำคนไข้กลับมารื้อวัสดุอุดเดิมออกแล้วบูรณะด้วยวัสดุที่แข็งแรง สวยงามมากขึ้น



ณ ปัจจุบัน คนไข้รายนี้ถอดเครื่องมือ ใส่เครื่องมือคงสภาพฟัน และกลับมาตรวจตามระยะ ยังคงสภาพการสบฟันตามปกติ ไม่มีปัญหาการปวดข้อต่อขากรรไกร แต่ยังไม่ได้บูรณะวัสดุฟันหน้าใหม่แต่อย่างใด


Orthodontic Case Review – The Crown Dental Clinic, KoratThis case involved a patient with a maxilla that was smaller than normal and V-shaped, combined with lower anterior teeth overlapping the upper anterior teeth (anterior crossbite). There was crowding of the anterior teeth in both the upper and lower arches, with the lower incisors tipped lingually even before treatment began. In addition, an impacted upper left canine was detected.All potential risks—both during orthodontic treatment and after treatment completion—were thoroughly explained to the patient. Fundamentally, this malocclusion was skeletal in origin. Ideally, the most definitive solution would have been orthognathic (jaw) surgery combined with orthodontic treatment, which would allow a more optimal and stable occlusion compared with orthodontic treatment alone. However, if the patient declined surgery, orthodontic treatment alone would inevitably carry certain risks, such as excessive lingual tipping of the lower anterior teeth or residual spaces. These issues might later require correction with composite build-ups or veneers after orthodontic treatment.Once the teeth were aligned and a stable occlusal relationship was achieved, planning focused on managing the remaining spaces resulting from extraction of severely crowded teeth. These spaces were temporarily managed with composite restorations during orthodontic treatment. After completion of orthodontic treatment, the patient was advised to return for removal of the provisional restorations and replacement with stronger and more esthetic definitive restorations.At present, the patient has completed orthodontic treatment, the appliances have been removed, and retainers are being worn. The patient returns for regular follow-up visits. The occlusion remains stable, with no temporomandibular joint symptoms, although definitive restoration of the anterior teeth has not yet been carried out.

ขอบคุณที่ติดตามอ่านบทความ : คุณหมอกอล์ฟ คลินิกทันตกรรมเดอะคราวน์โคราช